

How Do I Manage Heavy Periods From Fibroids?
You dread your period now. Not because of cramps, but because of what comes with them. Soaking through a pad and a tampon within an hour. Passing clots the size of a coin. Planning your week around proximity to a bathroom. Feeling completely wiped out by day two, not from pain but from blood loss.
This is not a normal period. This is fibroid bleeding. And it is one of the most physically and emotionally exhausting symptoms a woman can experience.
The good news is that you have real options. Heavy periods caused by fibroids are manageable, and in many cases, dramatically reducible, without immediately resorting to major surgery. Understanding those options clearly is the first step toward regaining control of your life.
Why Fibroids Cause Heavy Bleeding
Not all fibroids cause heavy periods. Size and location determine whether bleeding becomes a problem.
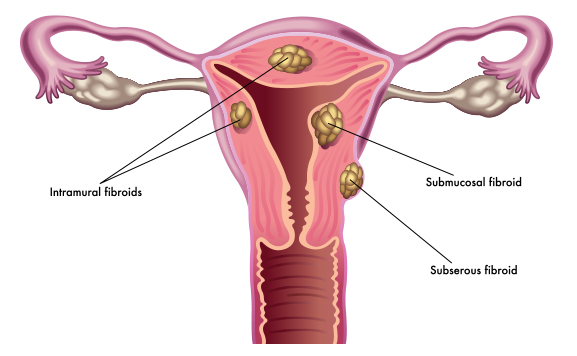
Submucosal fibroids, those that grow just beneath the inner lining of the uterus, are the most likely culprits. They directly disrupt the uterine lining, interfering with the body’s normal mechanisms for controlling blood flow during menstruation.
Intramural fibroids, which grow within the uterine muscle wall, also contribute to heavy bleeding when large. They prevent the uterus from contracting properly during your period, which is the main mechanism that stops blood flow. When the uterus cannot contract efficiently, bleeding continues longer and more heavily than it should.
Fibroids also increase the surface area of the uterine lining, which means more lining to shed each cycle. More lining equals more blood.
The result is periods that are heavier, longer, more clot-heavy, and more exhausting than anything you experienced before fibroids developed.
The Hidden Consequence: Iron Deficiency Anaemia
Before addressing how to manage the bleeding itself, this needs to be said clearly.
Chronic heavy bleeding from fibroids is one of the leading causes of iron deficiency anaemia in women of reproductive age. If your periods are consistently heavy, there is a very high probability that your iron stores are depleted, even if you feel like you are coping.
Anaemia caused by blood loss does not always feel obvious. It creeps up gradually. The fatigue starts to feel normal. The breathlessness when climbing stairs seems unremarkable. The inability to concentrate at work gets blamed on stress. The pale skin goes unnoticed.
If you have heavy fibroid bleeding, ask your doctor to check your full blood count and ferritin levels at your next appointment. Ferritin measures your iron stores, not just circulating iron, and it gives a more accurate picture of your actual reserves.
Treating anaemia alongside managing the bleeding is not optional. Leaving it unchecked slows your recovery, worsens fatigue, and makes every other symptom harder to manage.
Immediate and Short-Term Management
Tranexamic Acid
Tranexamic acid is a non-hormonal medication that reduces bleeding by helping blood clot more effectively at the site of the uterine lining. You take it only during your period, typically for the first three to four days of heavy flow.
Clinical trials show that tranexamic acid can reduce menstrual blood loss by up to 50% in women with heavy periods. It does not affect hormones, does not shrink fibroids, and does not interfere with fertility. For women who want immediate relief without hormonal intervention, it is often the first prescription option worth discussing with your doctor.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
NSAIDs like ibuprofen and naproxen reduce prostaglandins, the compounds that drive both period pain and increased blood flow during menstruation. Taken regularly at the start of your period, rather than only when pain becomes unbearable, they can reduce both cramping and blood loss modestly.
They are not as effective as tranexamic acid for heavy fibroid bleeding specifically, but they are accessible, affordable, and useful as a complementary measure.
Hormonal Management Options
The Hormonal IUD (Levonorgestrel-Releasing IUD)
The hormonal IUD, sold under brand names including Mirena, releases a low dose of the progestogen levonorgestrel directly into the uterus. Over time, it thins the uterine lining and, in many women, reduces or even stops menstrual bleeding entirely.
Research shows significant reductions in blood loss for women with fibroids using a hormonal IUD, though its effectiveness depends partly on fibroid size and position. It is not suitable for women with large submucosal fibroids that distort the uterine cavity, as this can prevent proper placement.
For women whose fibroids do not interfere with IUD insertion, it offers several years of continuous bleeding management with minimal systemic hormonal exposure.
Combined Oral Contraceptive Pill
The combined pill regulates hormonal fluctuations and can reduce period volume and duration. It does not shrink fibroids and is less effective than some other options for very heavy fibroid-related bleeding, but it is a reasonable management tool for women with moderate symptoms who also want contraception.
GnRH Agonists and GnRH Antagonists
These medications work by temporarily suppressing estrogen production, which causes fibroids to shrink and periods to stop or significantly reduce.
GnRH agonists like leuprolide are typically used short-term, for three to six months, often before surgery to shrink fibroids and reduce blood loss ahead of a procedure. Long-term use causes bone density loss and menopausal side effects, so they are not a standalone long-term solution.
GnRH antagonists like elagolix and relugolix are a newer class that work faster and have a more adjustable dosing profile. Relugolix combined with hormonal add-back therapy has strong clinical evidence for reducing heavy menstrual bleeding from fibroids and is now approved specifically for this use. It offers a meaningful non-surgical option for women who are not ready for or do not want a procedure.
Procedural Options That Preserve the Uterus
Endometrial Ablation
Endometrial ablation destroys the uterine lining using heat, cold, or energy. It significantly reduces or stops menstrual bleeding in most women. The procedure is minimally invasive, done as an outpatient, and has a relatively short recovery.
There are important caveats. Ablation is only appropriate for women who have completed their families, as it significantly reduces the chances of a successful pregnancy. It also works best for women with smaller fibroids. Large or numerous fibroids can make ablation less effective and increase the risk of incomplete treatment.
Uterine Fibroid Embolisation (UFE)
UFE is one of the most significant advances in fibroid management of the past two decades. A radiologist inserts a thin catheter into the femoral artery and guides it to the uterine arteries. Tiny particles are injected to block blood flow to the fibroids. Without a blood supply, the fibroids shrink and die.
UFE preserves the uterus, requires no general anaesthesia in most cases, and involves a recovery period of one to two weeks rather than the four to six weeks typical of major surgery. Studies show that 85 to 90% of women experience significant improvement in bleeding after UFE.
It is not recommended for women who want to become pregnant, and it is not suitable for all fibroid types or locations. A specialist assessment is essential to determine suitability.
Myomectomy
A myomectomy surgically removes individual fibroids while leaving the uterus intact. It is the gold standard for women who want to preserve their fertility while addressing heavy bleeding caused by fibroids.
It can be performed hysteroscopically for submucosal fibroids, laparoscopically for smaller fibroids, or via open abdominal surgery for larger or more numerous ones. The approach depends on fibroid size, number, and location.
Bleeding improves significantly after myomectomy for most women. Fibroids can recur over time, particularly in women who have had multiple fibroids or who are still in their early reproductive years.
Practical Daily Strategies While You Wait for Treatment
Managing heavy fibroid bleeding medically or surgically takes time. While you navigate the process, these daily strategies reduce the burden.
Use high-absorbency period products and combine options where needed, such as a tampon and a pad simultaneously on your heaviest days. Period underwear has become significantly more effective and is a genuinely useful backup layer.
Track your cycle carefully. Knowing when your heaviest days will arrive allows you to plan around them; scheduling lighter workloads, avoiding long journeys, and arranging your diary with proximity to bathrooms in mind.
If you pass large clots regularly, photograph them with your phone for scale and show them at your medical appointments. Many women under-report how much they bleed because they have normalised it. Concrete evidence helps your doctor take your symptoms seriously.
Rest without guilt during your heaviest days. Heavy blood loss is physically depleting. Treating your heaviest period days like recovery days is not laziness; It is appropriate self-care for a medical condition.
The Right Time to Push for More
If you are soaking through more than one pad per hour for two or more consecutive hours, that is medically heavy bleeding and warrants urgent medical attention. If your bleeding is impacting your ability to work, socialise, or function normally each cycle, that is not something to endure.
You have the right to effective treatment. Heavy periods from fibroids are not a life sentence. Push for the conversation, ask for the tests, and demand the options you deserve.